Finding Solutions: Increasing Autonomous Agency
 San Isidro medical campaign
San Isidro medical campaign
Gender inequality has manifested itself in many forms, in the fields of health and education most obviously and in less tangible but perhaps more complex arenas of social cohesiveness and power structures. My research interest throughout the semester has been driven by a curiosity of how to integrate the two realms in the context of my summer experience in rural Peru. More common is the tendency to focus on quantitative results from health and education initiatives because they are concrete and less messy to analyze. However, uncovering the explanations for some of the social determinants of health as I identified in Peru provides equally as much insight into solving health disparities as does data, perhaps even more so because of the humanist element that a qualitative social analysis retains.
What Does a Solution Mean?
It's extremely difficult to identify straightforward solutions to any of the issues I've raised, so perhaps steps for further research is the best direction to take in going forward. My topics of interest center around autonomy, specifically for women as it applies to the choices they make about their reproductive health.
I was able to observe many facets of women’s health in the clinics I volunteered in, from family planning to pregnancy to childbirth, and I paid close attention the interactions between health professionals and their female patients closely. A typical situation in the consult room was that women who were accompanied by a male relative or elder female relative did not speak for themselves when the obstetrician or doctor spoke to them; only when they came alone to the clinic did one-on-one conversation occur. The difference in behavior in both situations struck me as something that might be indicative of a larger force present in other areas of the women’s lives, areas in which they did not perceive themselves to have any power. Even more concerning to me was that the women who displayed such behaviors were part of the rural poor population who visited the clinics, not women who were gainfully employed or who lived in Otuzco proper. Such an issue does not provide a clear and simple path for resolving the layers of complexity surrounding it, but some lessons can be gathered from my preliminary research that may guide future exploration.
Reproductive Health: Emphasis on Females Alone?
Within the last ten years, some of the newest research at the intersection of social sciences and medicine recognizes the role that men have in reproductive health policies and power dynamics in the medical field, instead of solely focusing on women.
In 1994, the International Conference on Population and Development (ICPD) Programme of Action identified three paths through which men could have an improved role in female reproductive health, primarily through contraceptive use and family planning techniques, as well as support for female autonomy (Dudgeon and Inhorn 2004: 1380). The initial suggestions have straightforward implementations into apply in practice, through the combined efforts of physicians on the patient level and public health officials on the institutional level. However, the third suggestion is much more vague and requires the ethnographic works of anthropologists and sociologists in order to overturn existing power imbalances, or at least understand the culturally-bound limits on female autonomy.
The patriarchal social structures that pervade multiple levels of social interaction do not alone account for differences in reproductive health policies between genders, and the lack of complete understanding of the interplay between the two realms espouses a similar question to my initial one, that is how men’s reproductive health issues are ignored when directing so much energy to female health alone. I think students who are interested in reproductive health differences between genders, specifically in Peru, may find it more revelatory to go further into this area, devoting research to understanding how the political and economic history of Peru influenced reproductive health policies today.
What Does a Solution Mean?
It's extremely difficult to identify straightforward solutions to any of the issues I've raised, so perhaps steps for further research is the best direction to take in going forward. My topics of interest center around autonomy, specifically for women as it applies to the choices they make about their reproductive health.
I was able to observe many facets of women’s health in the clinics I volunteered in, from family planning to pregnancy to childbirth, and I paid close attention the interactions between health professionals and their female patients closely. A typical situation in the consult room was that women who were accompanied by a male relative or elder female relative did not speak for themselves when the obstetrician or doctor spoke to them; only when they came alone to the clinic did one-on-one conversation occur. The difference in behavior in both situations struck me as something that might be indicative of a larger force present in other areas of the women’s lives, areas in which they did not perceive themselves to have any power. Even more concerning to me was that the women who displayed such behaviors were part of the rural poor population who visited the clinics, not women who were gainfully employed or who lived in Otuzco proper. Such an issue does not provide a clear and simple path for resolving the layers of complexity surrounding it, but some lessons can be gathered from my preliminary research that may guide future exploration.
Reproductive Health: Emphasis on Females Alone?
Within the last ten years, some of the newest research at the intersection of social sciences and medicine recognizes the role that men have in reproductive health policies and power dynamics in the medical field, instead of solely focusing on women.
In 1994, the International Conference on Population and Development (ICPD) Programme of Action identified three paths through which men could have an improved role in female reproductive health, primarily through contraceptive use and family planning techniques, as well as support for female autonomy (Dudgeon and Inhorn 2004: 1380). The initial suggestions have straightforward implementations into apply in practice, through the combined efforts of physicians on the patient level and public health officials on the institutional level. However, the third suggestion is much more vague and requires the ethnographic works of anthropologists and sociologists in order to overturn existing power imbalances, or at least understand the culturally-bound limits on female autonomy.
The patriarchal social structures that pervade multiple levels of social interaction do not alone account for differences in reproductive health policies between genders, and the lack of complete understanding of the interplay between the two realms espouses a similar question to my initial one, that is how men’s reproductive health issues are ignored when directing so much energy to female health alone. I think students who are interested in reproductive health differences between genders, specifically in Peru, may find it more revelatory to go further into this area, devoting research to understanding how the political and economic history of Peru influenced reproductive health policies today.
|
Attitude Moving Forward
Improvement in the rate of maternal mortality in Peru provides a good example of how progress can be made in reproductive health. The Lancet reported in 2008 that the national rate of maternal mortality in Peru decreased significantly, and was attributed to a successful intercultural approach via the Mamawasi, a Quechua word describing a labor and birthing home for rural women in southern Peru. The Mamawasi brought some aspects of modern Western medicine to traditional, indigenous women, while still respecting their wishes to give birth in a home with family, away from the intimidating auspices of a hospital (Fraser 2008: 1233). That story exemplifies a poignant statement made by Paulo Freire: “No one knows it all; no one is ignorant of everything. We all know something; we are all ignorant of something” (1998: 39). Although originally spoken about teachers, his words ring very true for student-anthropologists to remember when engaging in international development studies. While foreign scholars and professionals can suggest solutions to issues they see as extremely serious in a developing nation, perhaps we are better off determining how change can be found locally, within the communities themselves. In terms of my project, alternative health policies and a stronger understanding, and later education, of gender and reproductive health by the population affected will result in the most effective change, regardless of what students from faraway locations may see or observe. After spending a semester researching the factors influencing the reproductive health issues I saw in my Peruvian health post and hospital, I understand that a combination of optimism and humility is key when making judgements on how to effect social change, especially when you as the student is not a true member of the community. |

San Isidro medical campaign
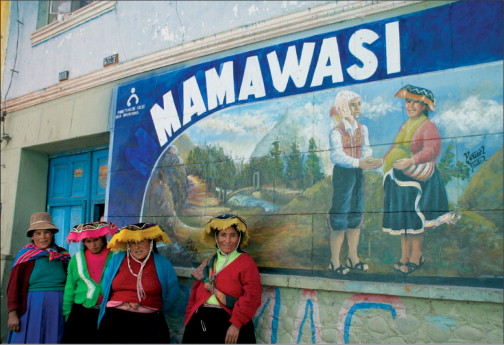
Photo credit: The Lancet
|
